
Anal Fistula Repair
Introduction
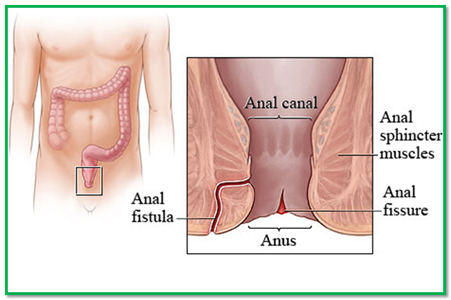
Some types of fistula have one channel, whereas others branch out into more than one opening. The fistula ends can appear as holes on the surface of the skin around the anus.
An anal fistula is painful and can cause bleeding when you go to the toilet.
Some fistulae can be connected to the sphincter muscles (the rings of muscles that open and close the anus).
When should I see Dr. B C Shah?
The common symptoms of an anal fistula include:
- skin irritation around the anus
- A throbbing, constant pain that may be worse when you sit down, move around, have a bowel movement or cough
- A discharge of pus or blood when having a bowel movement
You should see Dr. B C Shah if you have any of these symptoms.
What causes an anal fistula?
An anal fistula usually develops after an anal abscess (a collection of pus) bursts, or when an abscess has not been completely treated. A fistula can also be caused by conditions that affect the intestines, such as Crohn’s disease or ulcerative colitis.
As many as 50% of people with Crohn’s disease get an anal fistula. Up to 30% of people with HIV (a virus that attacks the body’s immune system) will also develop an anal fistula.
Anal fistulae are more common in men, mostly between the ages of 20 and 40.
Treating an anal fistula
Most anal fistulae require surgery because they rarely heal if they are not treated. Several surgical methods are available, depending on where and how complicated the fistula is.
You may be able to go home on the day of surgery. However, if the fistula is difficult to treat you may need to stay in hospital for a few days.
There is a risk of complications after anal fistula surgery, including:
- Infection
- Bowel incontinence
- The anal fistula coming back
For example, after the most common type of surgery for a fistula (known as a fistulotomy), the risk of an anal fistula coming back is around 21%. The risks vary depending on the type of procedure. You can discuss this with your Dr. B C Shah.
Symptoms of an anal fistula
There are several common symptoms of an anal fistula.
Symptoms include:
- Skin irritation around the anus (the opening where waste leaves the body)
- A throbbing, constant pain that may be worse when you sit down, move around, have a bowel movement or cough
- A discharge of pus or blood when you have a bowel movement
If your fistula was caused by an abscess that you still have, you may have:
- A high temperature of 38C (100.4F) or over
- Fatigue
- A general feeling of being unwell
If your fistula was caused by inflammation of the intestines (part of your digestive system), for example because of a condition such as irritable bowel syndrome or ulcerative colitis, you may also have:
- Abdominal pain
- Diarrhoea
- Loss of appetite
- Weight loss
- Nausea (feeling sick)
- Vomiting
Types of fistula
Anal fistulae are classified depending on their position and how close they are to the sphincter muscles. The sphincter muscles are two rings of muscles that open and close the anus. They are known as the internal and external sphincter muscles.
The most common types of anal fistula are:
- Intersphincteric fistula – the fistula tract (channel) crosses the internal sphincter and then opens on the surface of the skin next to the anus.
- Transsphincteric fistula – the fistula tract passes through both the internal and external sphincters and opens on the surface of the skin next to the anus.
Other types of anal fistula can:
- Begin at a different part of the colon (large intestine)
- Extend in a different direction, so that the fistula does not open next to the anus
- Develop in a horseshoe shape, with two open ends either side of the anus
Causes of an Anal Fistula
An anal fistula is most commonly caused by an anal abscess. It can also be caused by conditions that affect the intestines (part of your digestive system).
Anal abscess
An abscess is a painful collection of pus. An anal abscess usually develops after a small gland, just inside the anus, becomes infected with bacteria. The cause of the abscess is often unknown, although abscesses are more common in people with immune deficiencies, such as HIV and AIDS.
Abscesses are usually treated with a course of antibiotics (medication to treat infections caused by bacteria). In most cases, you will also need to have the infected fluid drained away from the abscess.
If an anal abscess bursts before it has been treated, it can sometimes cause an anal fistula to develop. A fistula may also occur if an abscess has not completely healed, or if the infected fluid has not been entirely drained away.
Approximately 40% of people with an anal abscess will develop an anal fistula.
Other causes
An anal fistula may also develop as a result of:
- A growth or ulcer (painful sore)
- A complication of surgery
- A health problem you were born with
Anal fistulae are also a common complication of conditions that cause the intestines to become inflamed, such as:
- Diverticulitis – the formation of small pouches that stick out of the side of the large intestine (colon), which become infected and inflamed
- Ulcerative colitis – a chronic condition that causes the colon to become inflamed and can cause ulcers to form on the lining of the colon
- Crohn’s disease – a chronic condition that causes inflammation of the lining of the digestive system
Other infections or conditions that can lead to the development of an anal fistula include:
- Cancer of the rectum – the rectum is an area at the end of the colon where faeces are stored
- Tuberculosis (TB) – a bacterial infection that mainly affects the lungs, but can also spread to many different parts of the body
- HIV and AIDS – a virus that attacks the body’s immune system (its defence against disease and infection)
- Chlamydia – a sexually transmitted infection that often causes no symptoms
- Syphilis – a bacterial infection that is passed on through sexual contact, injecting drugs or blood transfusions
Diagnosing an anal fistula
To diagnose an anal fistula, Dr. B C Shah will look at your medical history and carry out a physical examination. If there are several fistula tracts (channels), further tests may be needed to determine their position.
Dr. B C Shah will also pay particular attention to any history of anal abscesses or conditions that affect your bowels, such as Crohn’s disease. These conditions can lead to an anal fistula developing.
Physical examination
Dr. B C Shah will examine your anus (the opening where waste leaves the body) and the surrounding area for any physical signs of a fistula. The opening of a fistula usually appears as a red, inflamed (swollen) spot, which often oozes pus.
If the opening of the fistula is found, then he may be able to work out where the path of the fistula lies. The path of the fistula can sometimes be felt as a hard, cord-like structure beneath the skin.
Digital rectal examination
Dr. B C Shah will also perform a digital rectal examination(DRE). This involves placing a finger into your anus. During the DRE, the finger will be covered with a glove and lubricated with gel.
The DRE allows Dr. B C Shah to find out where the internal opening of the fistula is, and if there are any secondary tracts branching off it.
During the DRE, he may ask you to squeeze your sphincter muscles (the rings of muscles that open and close the anus) around their finger, to assess how well they are working.
The DRE will help determine what kind of treatment you need, or whether further tests are necessary.
Fistula probe
Dr. B C Shah may also need to use a proctoscope (special telescope with a light on the end) to see inside your rectum. They may also use a fistula probe, which is a tiny instrument inserted through the fistula.
These examinations may be performed under general anaesthetic, where you are asleep.
Further tests
If you have a complicated fistula with several branches, you may need further tests to determine the exact position of the fistula tracts. This will help determine your treatment.
Some further tests that may be recommended include:
- Anal endosonography (ultrasound) – this test uses high-frequency sound waves to create an image of the inside of your body. This is an accurate and frequently used way of locating the internal opening of a fistula.
- Magnetic resonance imaging (MRI) scan – an MRI scan uses strong magnetic fields and radio waves to produce a detailed image of the inside of your body. This type of scan is often used in cases of complex or reoccurring fistulae.
- Computerised tomography (CT) scan – a CT scan uses X-rays and a computer to create detailed images of the inside of your body. This may be used if you have an inflammatory bowel disease, such as Crohn’s disease, as it can be used to assess the extent of the inflammation.
Treating an anal fistula
Surgery is usually necessary to treat an anal fistula because very few will heal by themselves.
The aim of surgery is to heal the fistula while avoiding damage to the sphincter muscles (the ring of muscles that open and close the anus). Damage to the sphincter muscles could lead to bowel incontinence, where you do not have control over your bowels.
Surgery
Surgery for an anal fistula is usually carried out under a general anaesthetic, where you are unconscious and cannot feel anything. In some cases, a local anaesthetic is used, where you are conscious but the area being treated is numbed so that you do not feel any pain.
Some of the different types of anal fistula surgery are explained below. The type of surgery you have will depend on the position of your fistula. In all cases, Dr. B C Shah will be able to explain the procedure to you in more detail.
Fistulotomy
A fistulotomy is the most commonly used type of anal fistula surgery. It is used in 85–95% of cases of fistulae.
A fistulotomy involves cutting open the whole length of the fistula, from the internal opening to the external opening. Dr. B C Shah will flush out the contents and flatten it out. After one to two months, the fistula will heal into a flat scar.
To access the fistula, Dr. B C Shah may have to cut a small portion of the anal sphincter muscle. However, this will depend on the position of the fistula. Dr. B C Shah will make every attempt to reduce the likelihood of bowel incontinence.
Seton techniques
Dr. B C Shah may decide to use a seton during your surgery. A seton is a piece of surgical thread that is left in the fistula tract, often for several months, to keep the tract open. This allows it to drain properly before it heals.
This may be considered if you are at high risk of developing incontinence, for example because your fistula crosses your sphincter muscles.
It is also sometimes used to allow secondary tracts to heal before further surgery is carried out on the main tract. It can also be used to divide the sphincter muscle, which allows it to heal between operations.
If Dr. B C Shah is planning to use a seton, he will discuss this with you. In some cases, it may be necessary to have several operations to treat your fistula using seton techniques.
Advancement flap procedures
Advancement flap procedures may be considered if your fistula is complex, or if there is a high risk of incontinence.
An advancement flap is a piece of tissue that is removed from the rectum or from the skin around the anus.
During surgery, the fistula tract is removed (a procedure called fistulotomy). The advancement flap is then attached to where the internal opening of the fistula was.
Advancement flap procedures are thought to be effective in around 70% of cases.
Bioprosthetic plug
A bioprosthetic plug is a cone-shaped plug made from human tissue. It can be used to block the internal opening of the fistula. Stitches are used to keep the plug in place but the external opening is not completely sealed so that the fistula can continue to drain. New tissue then grows around the plug to heal it.
However, this procedure can sometimes lead to a new abscess forming or the plug being pushed out of place.
Two trials that used bioprosthetic plugs have reported success rates of over 80%. However, there is still uncertainty over the reoccurrence rates and long-term outcomes.
Non-surgical treatments
Fibrin glue
Fibrin glue is currently the only non-surgical option for treating fistulae. The fibrin glue is injected into the fistula to seal the tract. The glue is injected through the opening of the fistula, and the opening is then stitched closed.
Fibrin glue may seem an attractive option as it is a simple, safe and painless procedure. However, the long-term results for this treatment method are poor. For example, one small study had an initial success rate of 77%, but after 16 months only 14% of people were still successfully healed.
Ongoing research
Several clinical trials are currently taking place to compare the different types of treatment for anal fistulae, and you may be asked to take part in one.
If you are interested, you will be given information about the particular trial and you will be asked for your consent. Before giving your consent, make sure that you are fully aware of everything the trial involves, and feel free to decline if you do not wish to take part.
Recovering from surgery
After having surgery to remove an anal fistula, you should be able to move around and eat and drink after the effects of the anaesthetic painkilling medication have worn off.
If the fistula is relatively simple to operate on, you may be able to go home on the same day as the surgery. However, if the fistula is complicated, you may need to stay in hospital for a few days or have further surgery to complete the procedure.
Looking after the wound
After the operation, you will need to wear a dressing over the surgical cut until the wound has healed. A district nurse will visit you at home regularly to change the dressing and check how the wound is healing. Most wounds take around six weeks to heal.
There may be some bleeding or a discharge from the wound for the first few weeks, particularly the first time you have a bath or go to the toilet. You may wish to wear a pad, such as a sanitary towel, inside your underwear to avoid staining your clothes. This advice applies to both men and women.
You should see Dr. B C Shah if you have:
- Heavy bleeding
- Increasing pain, redness, swelling or discharge
- A high temperature of 38C (100.4F) or over
- Nausea (feeling sick) or vomiting
- Constipation (being unable to empty your bowels) for more than three days, despite using a laxative (see below)
- Difficulty passing urine
Painkilling medication
After the anaesthetic has worn off, you may need to take some pain relief medication. Over-the-counter (OTC) painkillers, such as paracetamol or ibuprofen, can normally be used, although you should check with Dr. B C Shah before using them. Always read the manufacturer’s instructions.
A 15-minute bath may also help to reduce the pain. The bath water should be as warm as you can comfortably sit in.
Antibiotics
You may be prescribed antibiotics (medication to treat infections caused by bacteria) to take before and after surgery. These will help reduce the risk of an infection. If you are prescribed antibiotics, make sure you complete the course.
Laxatives
Laxatives are a type of medicine that can help you empty your bowels. You may be prescribed laxatives to make it easier for you to go to the toilet after your operation.
Returning to normal activities
You may need rest for a few days after your operation, but you should avoid sitting still for a long time. Also avoid doing too much walking.
You can return to work and start to do some gentle exercise when you feel able to. Ask your Dr. B C Shah for advice on when you can drive again. Usually this is after a minimum of 48 hours. You should not go swimming until the wound has completely healed.
Complications of an anal fistula
Complications from an anal fistula are usually the result of fistula surgery. They can include infection, bowel incontinence or the fistula reoccurring.
Infection
Any type of surgery carries a risk of infection. If the fistula is not completely removed, for example because you are having the surgery carried out in several stages, an infection in the tract (channel) can sometimes spread to other parts of the body.
If this happens, you may require a course of antibiotics (medication to treat infections that are caused by bacteria). If the infection is severe, you may need to be admitted to hospital so that antibiotics can be administered through a drip in your arm (intravenously).
Incontinence
In some cases, surgery can damage the anal sphincter muscles (the ring of muscles that open and close the anus). If the muscles are damaged, you may lose control of your bowels, leading to faeces leaking uncontrollably from your rectum (the area where they are stored). This is known as faecal or bowel incontinence.
The likelihood of incontinence occurring after surgery will depend on the type of surgery you had and the position of your fistula. If you had some bowel incontinence before surgery, this may get worse.
Incontinence after a fistulotomy (surgery that opens up the fistula) is more common in women and in people with Crohn’s disease, a condition that causes inflammation of the lining of the digestive system. Rates of incontinence vary, although most studies report incontinence in between 3% and 7% of people.
After using seton techniques, the incontinence rate is 17%, and after an advancement flap procedure the incontinence rate is around 6–8%. Ask your Dr. B C Shah about the risks associated with your procedure.
Reoccurrence of the anal fistula
In some cases, the fistula can reoccur despite surgery. After having a fistulotomy, the reoccurrence rate is 21%. After an advancement flap procedure, the reoccurrence rate may be as high as 36%.
 Dr. Bimal Shah is the senior most General & Laparoscopic surgeon in Mira – Bhayandar with largest series of operations. He also consults at Borivali – Dahisar. He believes in ethical practice & is available at only trust hospitals. He passed out from KEM hospital, Mumbai in 1993 and was a lecturer training newer surgeons & medical students till 1998.
Dr. Bimal Shah is the senior most General & Laparoscopic surgeon in Mira – Bhayandar with largest series of operations. He also consults at Borivali – Dahisar. He believes in ethical practice & is available at only trust hospitals. He passed out from KEM hospital, Mumbai in 1993 and was a lecturer training newer surgeons & medical students till 1998. 






